Women and Children – Obstetrics and Gynaecology
About this leaflet
We advise you to take your time to read this leaflet, any questions you have please write them down on the sheet provided (towards the back) and we can discuss them with you at our next meeting.
It is your right to know about the operations being proposed, why they are being proposed, what alternatives there are and what the risks are. These should be covered in this leaflet.
This leaflet firstly describes what a posterior vaginal wall prolapse is, it then goes on to describe what alternatives are available within our trust, the risks involved in surgery and finally what operation we can offer.
What is a posterior vaginal wall prolapse
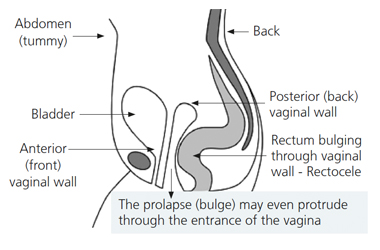
- Posterior means towards the back, so a posterior vaginal wall prolapse is a prolapse of the back wall of the vagina.
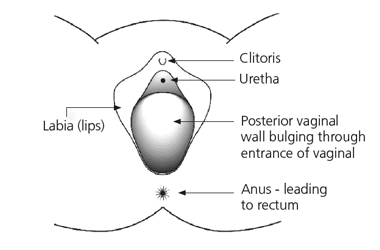
- Posterior vaginal wall prolapse is called a rectocele which describes the structure bulging into the vagina – the rectum (see diagram right).
- The pelvic floor muscles form a sling or hammock across the opening of the pelvis. These muscles, together with their surrounding tissue are responsible for keeping all of the pelvic organs (bladder, uterus, vagina, and rectum) in place and functioning correctly.
- Prolapse occurs when the pelvic floor muscles, their attachments or the vagina have become weak. This usually occurs because of the damage of childbirth but is most noticeable after the menopause when the quality of supporting tissue deteriorates.
- With straining, for example on passing a motion, the weakness described above allows the rectum (back passage) to bulge into the vagina and sometimes bulge out of the vagina (rectocele).
- A large rectocele may make it very hard to have a bowel movement especially if you have constipation.
- Some women have to push the bulge back into the vagina or support the perineal area (the area between the anus and the vagina) with their fingers in order to complete a bowel movement. Some women have to insert a finger in the back passage to facilitate evacuation of their bowel, this is called digitation.
- If a woman has difficulty in emptying the back passage or has to use her fingers to achieve bowel emptying, a special x-ray test to assess bowel emptying may be needed in planning the surgical approach.
The x-ray will involve inserting a special paste in the back passage and taking x-rays while trying to evacuate the paste from the back passage. - Some women find that the bulge causes a dragging or aching sensation.
Alternatives to surgery
- Do nothing
If the prolapse (bulge) is not distressing then treatment is not necessarily needed. If, however, the prolapse permanently protrudes through the opening to the vagina and is exposed to the air, it may become dried out and eventually ulcerate.Even if it is not causing symptoms in this situation it is probably best to push it back with a ring pessary (see below) or have an operation to repair it.
- Pelvic floor exercises (PFE)
The pelvic floor muscle runs from the coccyx at the back to the pubic bone at the front and off to the sides. This muscle supports your pelvic organs (uterus, vagina, bladder and rectum). Any muscle in the body needs exercise to keep it strong so that it functions properly. This is more important if that muscle has been damaged.PFE can strengthen the pelvic floor and therefore give more support to the pelvic organs. These exercises may not get rid of the prolapse but they make you more comfortable.
PFE are best taught by an expert who is usually a continence nurse advisor or women’s health physiotherapist. These exercises have no risk and even if surgery is required at a later date, they will help your overall chance of being more comfortable.
Types of pessary
Ring pessary
This is a soft plastic ring or device which is inserted into the vagina and pushes the prolapse back up. This usually gets rid of the dragging sensation and can improve urinary and bowel symptoms.
It needs to be changed every six to nine months, or earlier if there is any bleeding or discharge, and can be very popular; we can show you an example in clinic. Other pessaries may be used if the ring pessary is not suitable.
Some couples feel that the pessary gets in the way during sexual intercourse, but many couples are not bothered by it.
Shelf pessary or gellhorn
If you are not sexually active this is a stronger pessary which can be inserted into the vagina and again needs changing every four to six months.
General risks of surgery
- Anaesthetic risk
This is very small unless you have specific medical problems. This will be discussed with you. - Haemorrhage
There is a risk of bleeding with any operation. The risk from blood loss is reduced by knowing your blood group beforehand and then having blood available to give you if needed. It is rare that we have to transfuse patients after their operation. - Infection
There is a risk of infection at any of the wound sites. A significant infection is rare. The risk of infection is reduced by our policy of routinely giving antibiotics with major surgery. - Deep vein thrombosis (DVT)
This is a clot in the deep veins of the leg. The overall risk is at most four to five percent although the majority of these are without symptoms. Occasionally this clot can migrate to the lungs which can be very serious and in rare circumstances it can be fatal (less than one percent of those who get a clot).
DVT can occur more often with major operations around the pelvis and the risk increases with obesity, gross varicose veins, infection, immobility and other medical problems. The risk is significantly reduced by using special stockings and injections to thin the blood (heparin).
Specific risks of this surgery
- Damage to local organs
This can include bladder, ureters (pipes from kidneys to the bladder) and blood vessels. This is a rare complication but requires that the damaged organ is repaired and this can result in a delay in recovery. It is sometimes not detected at the time of surgery and therefore may require a return to theatre. If the rectum (back passage) is inadvertently damaged at the time of surgery, temporary colostomy (bag) may be required but this is exceptionally rare. - Prolapse recurrence
If you have one prolapse, the risk of having another prolapse sometime during your life is 30%. This is because the vaginal tissue is weak. - Pain
General pelvic discomfort, this usually settles with time but occasionally pain on intercourse may occur and can sometimes be permanent. - Reduced sensation during intercourse
Sometimes the sensation during intercourse may be less and occasionally the orgasm may be less intense. In rare circumstances the vagina may become too narrow so that intercourse cannot take place. Corrective surgery may be complex but could be an option in the circumstance. - Change in bowel function
Occasionally patients can become constipated after the operation but often bowel function is improved.
Posterior vaginal wall prolapse repair
Following the operation you are likely to feel more comfortable. Intercourse may be more satisfactory. Opening your bowels may be easier, but this can not be guaranteed.
Before the operation
It is recommended that you take a medication to soften your motions for at least three days before the operation. This will help to reduce the risk of you getting constipated after the operation and could mean you get home earlier. Magnesium sulphate, Lactulose or Movicol would be suitable and you can obtain these from your GP. If you are post-menopausal your Gynaecologist may recommend local oestrogen cream.
How the operation is performed
- The operation can be done with a spinal or general anaesthetic. You may have a choice of which anaesthetic is used.
- A spinal anaesthetic involves an injection in the lower back, similar to what we use when women are in labour or for a caesarean section. The spinal anaesthetic numbs you from the waist down. This removes any sharp sensation but a pressure sensation will still be felt.
- A general anaesthetic will mean you will be asleep (unconscious) during the entire procedure.
- The legs are placed in stirrups (supported in the air).
- The back vaginal wall is numbed with local anaesthetic.
- A horizontal cut is made where the back wall of the vagina meets the skin just outside the vagina.
- A vertical cut is then made in the back wall of the vagina, over the area of the bulge – Figures 1 and 2.
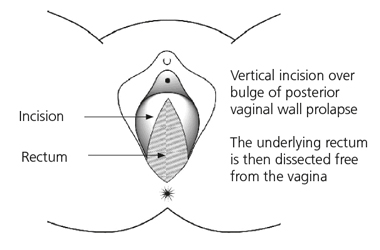
- The vaginal skin is then separated from the rectum (lower bowel).
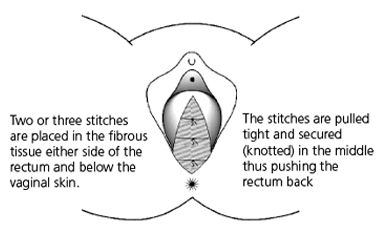
- Two or three stitches are placed in tissue at either side of the rectum.
- These stitches are then tied in the centre thus bringing the tissue into the middle so that the rectum is held behind them and thus supported. This then stops the rectum bulging into the back vaginal wall – Figure 3.
- Sometimes a perineorrhaphy, which is a surgical repair of the perineum (the skin and muscle between the front and back passage), will be performed. This can improve the prolapse repair but can result in tightening of the vaginal entrance and pain during sexual intercourse.
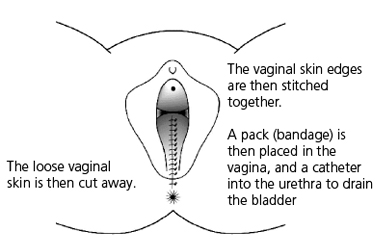
- Any excess vaginal skin is trimmed and then the vaginal skin closed with stitches – Figure 4.
- A vaginal pack (ribbon gauze to apply pressure) may then be inserted into the vagina which is removed the following morning. A catheter may also left in the bladder overnight.
After the operation: in hospital
- On return from the operating theatre you will have a fine tube (drip) in one of your arm veins with fluid running through to stop you getting dehydrated.
- You may have a bandage in the vagina, called a ‘pack’ and a sanitary pad in place. This is to apply pressure to the wound to stop it oozing.
- You may have a tube (catheter) draining the bladder. The catheter may give you the sensation as though you need to pass urine but this is not the case.
- Usually the drip, pack and catheter come out the morning after surgery or sometimes later the same day. This is not generally painful.
- After this operation some patients go home the same day
- If you are still in hospital the day after the operation you will be encouraged to get out of bed and take short walks around the ward. This improves general wellbeing and reduces the risk of clots in the legs.
- You may be given injections, to keep your blood thin and reduce the risk of blood clots in your legs.The injections are normally given once a day until yougo home, or longer in some cases.
- The wound is not normally very painful but sometimes you may require tablets or injections for pain relief.
- There will be slight vaginal bleeding like the end of a period after the operation. This may last for a few weeks.
- The nurses will advise you about sick notes, certificates etc. You may be in hospital for up to four days.
After the operation: at home
- Moving is very important; using your leg muscles will reduce the risk of clots in the back of the legs (DVT), which can be very dangerous.
- You are likely to feel tired and may need to rest in the daytime from time to time for a month or more, this will gradually improve.
- It is important to avoid stretching the repair particularly in the first weeks after surgery. Therefore, avoid constipation and heavy lifting. The deep stitches dissolve during the first three months and the body will gradually lay down strong scar tissue over a few months..
- Do not use tampons for six weeks.
- There are stitches in the skin wound in the vagina. Any stitches under the skin will dissolve by themselves. The surface knots of the stitches may appear on your underwear or pads after about two weeks, this is quite normal. There may be little bleeding again after about two weeks when the surface knots fall off, this is nothing to worry about.
- At six weeks gradually build up your level of activity.
- After three months, you should be able to return completely to your usual level of activity.
- You should be able to return to a light job after about six weeks, a busy job in 12 weeks. Avoid all unnecessary heavy lifting.
- You can drive as soon as you can make an emergency stop without discomfort, generally after three weeks. You must check this with your insurance company, as some of them insist that you should wait for six weeks.
- You can start sexual relations whenever you feel comfortable enough after six weeks, so long as you have no blood loss. You will need to be gentle and may wish to use lubrication (KY jelly) as some of the internal knots could cause your partner discomfort. You may, otherwise, wish to defer sexual intercourse until all the stitches have dissolved, typically three to four months.
- Follow up after the operation is usually six weeks to six months. This maybe at the hospital (doctor or nurse), with your GP or by telephone. Sometimes follow up is not required.
Avoiding constipation
Drink plenty of water or juice
Eat fruit and green vegetables especially broccoli
Plenty of roughage, for example; bran or oats
Information about the British society of urogynaecology surgical database (surgical register)
The British Society of Urogynaecology (“BSUG”) is a national group of gynaecologists with a special interest and expertise in the treatment of incontinence and prolapse. BSUG has developed a database of clinical and surgical data for the purposes of publishing anonymous statistical information for research purposes and to enable individual NHS Trusts and consultants to audit information about operations to ensure that the procedures performed at their hospitals are as safe and effective as possible.
The patient information held in the BSUG database comprises name, hospital number and date of birth, together with clinical and surgical information (“patient identifiable data”). Because this information is confidential to each patient and is that patient’s personal data within the meaning of the Data Protection Act 1998,we do not disclose patient identifiable data to BSUG without written consent.
The benefits the BSUG database may bring to you:
Improving patient awareness of the outcomes of incontinence and prolapse surgery
Finding out how long the different operative procedures last
Helping to identify individual patients who have received an implant and where there may be a need for urgent clinical review
The BSUG database will also be used to bring additional long-term benefits by:
Providing feedback to gynaecological surgeons and teams to help maintain high clinical standards
Promoting open publication about the performance of implants used in operations.
Providing feedback on implant performance to regulatory authorities
Providing feedback to suppliers about the performance of their implants
Monitoring and comparing the performance of hospitals
Data collection – its security and confidentiality
The BSUG database uses an electronic system for data collection. The data is sent securely to a protected database, avoiding the need to send paper records through the post, to ensure your data receives maximum protection.
Your personal information is confidential and cannot be used outside of the BSUG database. Strict procedures are in place to protect your information and keep it confidential; it will only be available to you and your surgeon. If you wish, you can obtain access to a copy of your own record in accordance with the Data Protection Act 1998.
BSUG database consent
I consent to:
- The processing of my patient identifiable data for the research and auditing purposes described in this information sheet.
- The disclosure by BSUGs of my patient identifiable data to its IT service provider or any future IT service provider, where such IT service provider has:
(a) Agreed to adopt appropriate technical and organisation measures to protect the
security of my patient identifiable data and only to process it in accordance with
BSUGDL’s instructions;
(b) Been instructed NOT to store my patient identifiable data on a server which is
located outside of the United Kingdom; and
(c) Been informed of the existence of my legal right to confidence in respect of my
patient identifiable data. - The disclosure of my patient identifiable data to the consultant team (and the NHS Trust employing that consultant team) who disclosed it to BSUG.
- The disclosure of my patient identifiable data to BSUG or any legal entity which is wholly owned by BSUG, for processing in accordance with the consents in this section.
Your participation is voluntary
The form asks for your consent for your personal information to be recorded by the BSUG database.
Your participation in the BSUG database is entirely voluntary. You can request access to view your entry on the BSUG database from your consultant team.
If you agree and then change your mind, you may revoke this permission at any time by sending a written notice to your consultant OR to the address below. If you do not agree, your data will not be entered.
BSUG Database Limited
c/o BSUG
Royal College of Obstetricians and Gynaecologists
27 Sussex Place
Regents Park
London
NW1 4RG
If you consent to the above please sign in the relevant section on the operation consent form.
Things I need to know before I have my operation
| Please list below any questions you may have, having read this leaflet. |
| Please describe what your expectations are from surgery. |
Patient experience
South Tees Hospitals NHS Foundation Trust would like your feedback. If you wish to share your experience about your care and treatment or on behalf of a patient, please contact The Patient Experience Department who will advise you on how best to do this.
This service is based at The James Cook University Hospital but also covers the Friarage Hospital in Northallerton, our community hospitals and community health services.
To ensure we meet your communication needs please inform the Patient Experience Department of any special requirements, for example; braille or large print.
T: 01642 835964
E: [email protected]