What is a metastatic spinal cord compression (MSCC)?
The spinal cord is a bundle of nerves that runs from the brain and to the lower part of the back, and has important roles in functions such as movement, bladder and bowel functioning, sensations of touch, pain, and temperature.
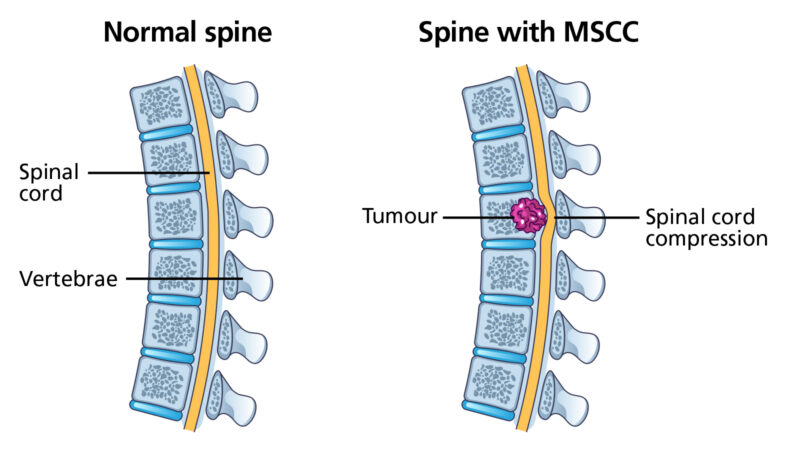
Spinal cord compression occurs when there is pressure on the spinal cord, which can stop the nerves functioning normally. This can occur when cancer grows in the bones of the spine or in surrounding tissues of the spinal cord.
MSCC is rare, between 5 to 10% of cancer patients develop a spinal cord compression. The most common types of cancers that can spread to the bone is prostate, lung, and breast cancer.
If MSCC are not diagnosed/treated urgently, damage to the spinal cord can lead to permanent paralysis.
Metastatic spinal cord compression- red flag symptoms
Please see below the list of some of the common signs and symptoms which patients diagnosed with MSCC have reported.
Diagnosing and early treatment is crucial to improve a patient’s quality of life with MSCC.
It is important to note that having some of these symptoms does not necessarily mean a diagnosis of MSCC, however reporting of symptoms and investigations are essential to come to a diagnosis.
Metastatic spinal cord compression (MSCC) key red flags
- Past medical history of cancer (note 25% of patients do not have a diagnosed primary)
- Early diagnosis is essential – as the prognosis is severely impaired once paralysis occurs
- A combination of red flags increases suspicion – the more red flags the higher the risk and the greater the urgency
Credit: The above information has been produced by The Christie NHS Foundation Trust. The Greater Manchester and Cheshire MSCC guidelines can be accessed on The Christie NHS Foundation Trust website.
Early warning signs of MSCC
The following has been produced by Greenhalgh S, Turnpenny J, Richards L, Selfe J (2010)
- R– Referred back pain is multi-segmental or band-like
- E– Escalating pain which is poorly responsive to treatment (including medication)
- D – Different character or site to previous symptoms
- F – Funny feelings, odd sensations or heavy legs (mult-segmental)
- L – Lying flat increases back pain
- A – Agonising pain causing anguish and despair
- G – Gait disturbance, unsteadiness, especially on stairs (not just a limp)
- S – Sleep grossly disturbed due to pain being worse at night
NB – established motor, sensory, bladder, bowel disturbances = late signs
What to do:
If you suspect or have any concerns your patients may have MSCC, it is important to act quickly in order to ensure the best outcome can be achieved.
- Arrange an Urgent Whole Spine MRI with urgent reporting (if the scan is not performed a JCUH, ask for images to be sent to JCUH PACS as soon as possible). If there is any contraindication against having an MRI, a CT of the whole spine (sagittal slice) should be completed.
- Steroids: start 16mg OD (or 8mg BD) of dexamethasone (with PPI cover (gastric cover) (unless contraindicated).
- If impending or confirmed MSCC is reported:
-First refer to Oncology for urgent assessment/radiotherapy treatment via Webice (Urgent Radiotherapy Referral) or external referral form.
-Discussion with oncology to assess if referral for spinal surgery is appropriate via the hospitals spinal referrals (patient pass).
– If the patient has no previous diagnosis of cancer. Please contact the on-call Consultant/Registrar for advice.
Further advice
- If not previously known to oncology/ Admit: Admit to local A&E if patient is in the community (highlight suspicion of MSCC) and monitor neurology until results are back and referral has been reviewed.
- Spinal Instability: If severe pain on mobilising/problems with standing and mobility- patient should have bed rest and be immobilised in a comfortable position (flat or semi reclined). If patient has some spinal pain but is mobilising comfortably then they should be allowed to do so.
- Radiology: Referring practitioner to request urgent MRI and state on referral ‘Suspected MSCC” with a description of presenting signs and symptoms. Follow this with a phone call to MRI department to make radiology team aware.
Important contacts for radiotherapy andoncology
Sophie Burns: Advanced practitioner in palliative radiotherapy
- Mobile- 07442824652
- Available: Monday to Friday, 9am to 5pm.
- (Outside these hours, please contact the on-call consultant/registrar).
On-call oncologist, consultant or registrar
- Phone The James Cook University Hospital switchboard, 01642 850850, and ask for the oncology consultant or registrar on-call.
- (For after hours Monday-Friday and including weekends and bank holidays)
Acute oncology service (AOS) The James Cook University Hospital
- Mobile: 07741616475
- Tel: phone 01642 850850 and enter extension 57983
- Email: [email protected]
- Available: Monday to Friday, 9am to 5pm.