Women and Children – Obstetrics and Gynaecology
Even if your surgeon has explained to you what the operation entails many of us do not take in everything mentioned in the clinic, so this information is to help you understand your condition and the reason for the intended treatment.
As we are all different, it is not possible to personalise this information, so there may be differences between your individual case and the information given here.
If you have any queries regarding the information please discuss them with the consultant or a member of their team (doctors or nursing staff).
Why do I need a laparotomy?
You have been found to have a mass or lump in your pelvis. At this point we do not know the diagnosis (exact cause) of this mass and the only way to be certain is to do this operation, remove the mass and send it to the laboratory to be looked at under a microscope.
There are several possibilities, it may be a benign (harmless) ovarian cyst or mass, a borderline cancer, or it may be coming from one of the other organs in the pelvis such as the bowel or the womb, for example fibroids. It may be an ovarian cancer.
What is ovarian cancer?
The ovaries are the female reproductive organs which contain the ova (eggs). Ovaries also release the female hormone oestrogen, which helps support pregnancy and contributes to female sexual characteristics.
A gradual decline in oestrogen production normally takes place in women between the ages of 48 and 52. At the same time, the monthly release of eggs decreases and the menstrual cycle becomes irregular and eventually stops. This is called menopause.
The ovaries, like other body parts, are made up of tiny cells. Normally, cells divide and reproduce themselves in a controlled manner. In cancer this process gets out of control and the cells continue to divide developing into a lump which is called a tumour. If untreated it may invade and destroy surrounding tissue.
Ovarian cancer is difficult to diagnose because the symptoms are vague. There may be abdominal enlargement, usually due to fluid building up. Some women experience a change in bowel function, urinary frequency, and, or nausea. In some cases, ovarian cancer initially causes no symptoms and is discovered incidentally during a pelvic examination.
What is a laparotomy?
A laparotomy is an exploratory operation.
The surgeon opens the abdomen (tummy), starting at the top of the pubic hairline and going up to, and sometimes above, the umbilicus (belly button).
What does the operation involve?
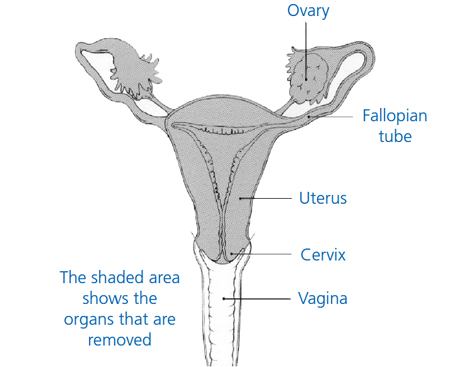
The exact operation depends on what we find. Usually it will involve removal of both ovaries and tubes and removal of the uterus (womb), known as a hysterectomy and removal or biopsies of any other suspicious areas.
Often we also remove the omentum – this is a pad of fat (like a baby’s bib) that is attached to part of the large intestine, and is a common place for ovarian cancer to spread to.
The extent of the surgery depends on how concerned we are about the risk of cancer and on how much the cancer, if present, has spread. If cancer is found, as much of the tumour as possible is removed. In some cases it is only possible to remove a small amount of the tumour.
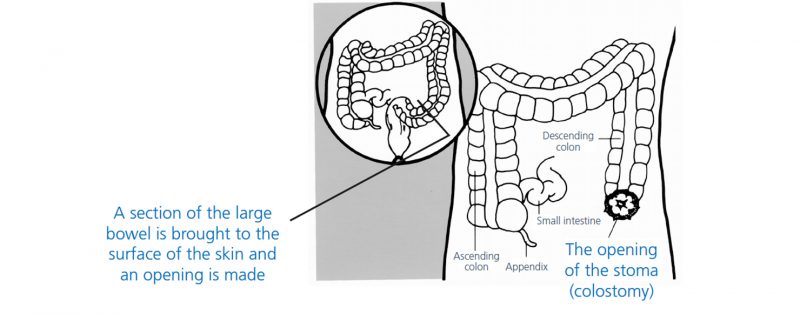
Ovarian cancer can sometimes require bowel surgery, and the surgeon may make an opening in the abdominal wall to pull through and open a section of the large bowel.
This opening is often called a stoma or colostomy. A pouch is placed over the stoma to collect the waste products that would usually pass through the bowel and out of the body through the rectum and anus (your back passage).
While this is very worrying, most patients do not need this type of surgery.
Are there any alternatives to a laparotomy?
Do nothing
Sometimes patients choose not to have a laparotomy. This can be a risk as without a proper diagnosis, no treatment can be given and any cancer present could continue to grow and spread whilst nothing was being done.
A biopsy of the mass
This can sometimes be done but can also cause problems and is usually only done if the doctor does not think you are fit for surgery or if the tumour cannot be removed safely. If the biopsy shows the tumour is cancer then chemotherapy can be used to try and control the disease.
Are there any complications or risks associated with a laparotomy?
We know there may be complications following various gynaecological operations or procedures, that are not particularly serious but do happen more often.
These frequently occurring risks include: Pain, bruising, delayed wound healing, scarring of the skin or scar tissue inside (adhesions). Numbness, tingling or burning sensation around the scar which may take weeks or months to resolve. Anaemia, fatigue or tiredness. Urinary frequency or loss of control.
Wound infection, urinary tract infection or chest infection which is usually easily treated with antibiotics. Patients are encouraged to follow the recommended post-operative breathing exercises and to stop smoking.
Are there any ‘more serious’ risks?
There can be other complications following any gynaecological operation. Whilst these don’t happen often when they do occur they can be serious. It is known some risks are increased if you already have underlying medical problems or if there is scar tissue (from previous operations or disease) which makes the hysterectomy more difficult. The risks are also increased if you are obese or if you smoke. The more serious risks include:
Infection
This may occur in the pelvis, bladder, vagina, incision site or in the chest. Infections are usually easily treated with antibiotics but occasionally an abscess may form in the pelvis which may require surgical drainage under anaesthetic. All ladies having laparotomy are given antibiotics pre-operatively to help prevent infection.
Bleeding
This may occur during the operation or, rarely, afterwards and may be enough to need a blood transfusion. If you have had some internal bleeding and we find blood has collected in your pelvis, we call this a haematoma. A haematoma can usually be easily treated with antibiotics to encourage the blood to drain out through your vagina, but occasionally it may need to be drained surgically under anaesthetic.
A haematoma is often described as a blood clot, and this is quite a good description but must not be confused with the blood clots described in section four.
Visceral injury
This means injury to the bowel, bladder or ureters (the two tubes coming from the kidneys into the bladder).
These complications would usually be found during the operation and dealt with immediately. In rare cases the problem may not become apparent for a few days after the operation and this may require a second laparotomy to resolve the problem.
Venous Thromboembolism
There are two types:
Deep vein thrombosis (DVT)
Following a laparotomy, it is possible for clots of blood to form in the deep veins of the legs and pelvis. If this does occur, a deep vein thrombosis would cause pain and swelling in a leg and can be treated relatively simply with drugs.
The risk of developing a DVT is minimal, as many precautions are taken to help prevent and minimise the risks such as:
- Recommending you reduce or stop your smoking in the weeks before your operation
- The use of support stockings and, or medication to ‘thin the blood’
- The use of special equipment in the operating theatre
- The recommended post-operative leg exercises
Pulmonary embolism
In rare cases, it is possible for a clot to break away and be deposited in the lungs and if this occurs it is a serious situation and will need immediate treatment with drugs. The precautions against pulmonary embolism are the same as for DVT.
If you do have any concerns about the risk of complications, please discuss them with the consultant or a member of their team (doctors or nursing staff) and your questions will be answered as clearly and as honestly as possible.
What happens before the operation?
For this operation, you will be taking part in an enhanced recovery programme with the aim of helping you recover quickly and safely. During your short stay in hospital there will be goals which you will be encouraged to achieve.
A team of doctors, nurses, physiotherapists and other healthcare professionals will be monitoring your progress and will support you in reaching your goals so in most cases you will be asked to attend a pre-admission session shortly before you are due to have your operation.
You will be seen by a nurse who will begin your plan of care. The nurse will also review your medical history. You will have your weight and height, blood pressure and pulse and some blood samples taken. Depending on your age or medical history you might also be requested to attend other departments on the same day for investigations such as an ECG – Electocardiogram (heart tracing), a lung function test or a chest X-ray.
You may also need to see a doctor for a more detailed medical examination. You will need to take all your medicines to pre-admission with you as most should be continued before your operation and throughout your hospital stay but some may need to be stopped to reduce any risks and to avoid your operation being delayed or cancelled.
If it is felt that you will require bowel surgery you will meet the specialist nurses who will give you advice and mark you tummy in case this is required.
This is also an opportunity for you to tell us about your own individual needs and circumstances. It is our aim for you to have a speedy recovery and safe discharge so it is important you tell us as early as possible if you have any concerns about whether or not you will be able to manage your daily activities when you go home.
You may wish to bring along a relative or close friend to pre-admission who can also be involved and support you in planning your enhanced recovery. You will have the opportunity to ask the nurse any questions.
Your anaesthetist would prefer you to stop cigarette and cannabis smoking in the weeks before your operation, as this is known to increase the risk of anaesthetic complications, for example; breathing difficulties, coughing, nausea and sickness and chest infection.
On the day before your operation you will be able to eat and drink as normal but please avoid drinking alcohol on the evening before your operation as this may lead to dehydration.
To reduce the possibility of skin infection, we request you do not shave your bikini-line or your legs during the week before your operation but some ‘trimming back’ of excess pubic hair may be required, you can do this yourself at home or the nursing staff will help you after you are admitted.
A key aspect of the enhanced recovery programme is that you will be given clear carbohydrate drinks before your surgery. These drinks will help to give you the much needed energy which you will require to help you recover.
Most of the time your admission date will be confirmed at pre-assessment, as it may be necessary for you to be admitted the day before your operation.
Admission into hospital
- Usually you will be admitted on the day of your surgery, you will recieve a letter with instructions where to go, what time and when to stop eating or drinking.
- Do not suck sweets or chew gum.
- You will need to take a bath or shower at home and take off as much of your jewellery as possible although we are able to cover wedding rings/bangles if you are unable to remove them. Please remove any nail varnish or false nails.
- If you are admitted the day before your operation, the nursing staff will help and advise you about the above.
- To reduce the possibility of any damage to your eyes, it is very important you remove all mascara and wear glasses instead of any type of contact lenses. Please wear comfortable clothes that are not tight around the waist.
- You will need to bring a packet of sanitary towels into hospital with you, toiletries, dressing gown, nightgown and slippers, and you may also choose to bring in a book or magazine.
Please read your admission letter carefully to see where you are being admitted to. If you are unsure, you may phone the nursing staff as follows:
- Gynae Oncology Specialist Nurses 01642 282418
- The Surgical Admissions Unit at The James Cook University Hospital: 01642 854603
What can I expect on the operation day?
If you have not already signed your consent form for the operation, you will be seen by your consultant or a member of their team who will explain your operation in detail and answer any questions you may have. You will then be required to sign the consent form.
Because of the extent of the surgery it may be advised that you have a spinal or epidural anaesthetic. This will depend on discussion between you and your anaesthetist. You will still be sedated but a spinal (epidural) may be advised to aid a speedy recovery and pain management.
The nurses will give you ‘support socks’ and a small injection may be given to thin the blood, helping to reduce the risk of a blood clot developing in your legs during the operation. You will then be transferred to the theatre area by a nurse and or porter.
What can I expect after the operation
When the operation is completed you will be woken by the anaesthetist and transferred, on your trolley, to the recovery area in theatre. Your recovery nurse will look after you and stay with you until they are satisfied with your condition.
You will be transferred to the ward on your trolley and the ward staff, with the help of the theatre porter, will transfer you into your bed. You will probably feel drowsy for a few hours afterwards.
To enhance your recovery it is important you start doing the recommended breathing exercises, as described in the back of this booklet, as soon as you wake up.
You are likely to have a ‘drip’ (also known as an I.V.) to give you intravenous fluids. The morning after your operation you will be able to start drinking and you may even have something to eat if you are not feeling sick. It is important you eat and drink early after your operation so we will encourage you to have normal food as well as nourishing drinks which will be available for you while you are in hospital.
Effective pain and sickness control is an important part of the enhanced recovery programme as this will allow you to start walking around, breathe deeply, eat and drink, feel relaxed and sleep well.
Pain and sickness may be controlled with a PCAM machine (Patient Controlled Analgesia Monitoring) allowing you to control the amount of pain relief and anti-sickness drugs that you have and should result in a comfortable recovery.
You may also have 2 pain quells inserted into the wound for localized pain relief. If you do have quills or a PCA it will be removed once you are able to tolerate painkillers by mouth, or in suppository form, usually within 24/48 hours of the operation.
You may have a catheter inserted into your bladder. This will drain your urine and will remain in place until you are fully mobile and able to pass urine normally.
What can I expect in the days after the operation?
To enhance your recovery you may be visited by the physiotherapist the day after your operation. She will give you advice on gentle post-operative exercise and a leaflet to read.
You will be encouraged to increase your mobility gradually during the day after your operation until you can be fully mobile making it possible for you to have a shower or to go in the bath, with some assistance from the staff.
You may feel much more tired than usual after your operation as your body is using a lot of energy to heal itself so you may need to take a nap for the first few days.
A laparotomy for an abdominal mass can also be emotionally stressful and many women feel tearful and emotional at first – when you are tired these feelings can seem worse. For many women this is often the last symptom to improve.
It usually takes a few days before your bowels start to work normally and you may experience discomfort associated with a build-up of wind. This usually resolves itself, but if it becomes a problem the nursing staff may encourage taking gentle exercise.
It is important to keep your genital area and any abdominal wounds clean. A daily bath or shower is advisable paying particular attention to these areas. Avoid the use of highly scented soaps, bubble bath and vaginal deodorants, etc. We will provide a sterile dressing to cover the wound after bathing.
If dressings are still needed on discharge they will be provided by the nursing staff.
You may have dissolving stitches in your wound, in which case you will be advised by the nursing staff how to care for them. If you have clips, staples or sutures (stitches) which need to be removed, the nursing staff will explain how to care for your wound and advise you when they will be removed.
You should expect to have some vaginal bleeding in the first few days after the operation. The bleeding normally turns into a red or brownish discharge before stopping completely and can last anything from a few days to a few weeks.
We advise you to use sanitary towels in preference to tampons whilst the bleeding persists, as this will help you to keep a check on the amount you are losing and will help to reduce the risk of infection associated with tampon use.
Some further, slight, bleeding may occur about four to six weeks after your operation. This can happen because your internal stitches are dissolving. As long as this bleeding only lasts for a day or two do not worry, but if it becomes very heavy and you are worried, please contact your GP.
How long can I expect to be in hospital after the operation?
Many patients feel well enough to leave hospital one to three days after the operation but you must tell your nurse how you are feeling and she will help you to decide whether you are ready.
Will I get any medication to take home on discharge?
You will take home the medicines you brought in with you. We will provide any extra medicines you may need, such as painkillers or antibiotics, from the hospital pharmacy. Please stock up on Paracetamol and ibuprofen if you are able to tolerate these as we do not provide them on discharge.
We usually provide some laxatives as constipation can be a problem post op and 28 days of Low molecular weight heparin injections to thin the blood to help prevent deep vein thrombosis, pulmonary embolus. The nurses will discuss administration of the injections on discharge.
You will still require dressings, this will also be organised from the ward.
How will my care continue?
After your operation, the tissues taken away will be fully analysed then discussed at our Multidisciplinary Team (MDT) meeting and this may take up to four weeks.
We will have asked you, at pre assessment, how you would like to receive your results, either by a formal visit to the out-patients clinic or by a telephone call from the specialist nurse.
If you have any questions, please ask any of the team looking after you – we are happy to help.
Contact us
If you need to contact us, please feel free to do so. The Cancer Nurse Specialist is happy to speak to you at any time.
Her number is 01642 282418.
If she is not there, an answerphone is available.
What happens if I do have ovarian cancer?
If you do have ovarian cancer, then you may need further treatment. This is drug treatment, ‘chemotherapy’. We will discuss this in detail with you if it is necessary. If you do not need further treatment we may make arrangements to see you back in the clinic after about two months to make sure that there are no further problems.
You will be followed up in the gynaecology or oncology clinic for five years following your surgery. Follow-up is three monthly, then four monthly, then six monthly, then yearly, but always remember if you have any problems contact your GP.
What happens when I go home?
You will go home wearing the support stockings you were given and are advised to wear them for at least six weeks until you are back to your full mobility. Please wear continuously for the first 2 weeks and then on an evening or when your not mobile for the last 4 weeks.
Many women lose their interest in sex during cancer treatment. Any form of surgery can affect our sex lives. During the operation the surgeon removes part of the vagina, reducing its length, but once the scars heal this is not usually a problem.
Early on whilst the surgery scars heal it is not advisable to have penetrative sex (three to four weeks). The surgery should not affect a woman’s ability to have an orgasm if this is a normal experience during sexual activity.
If you experience any discomfort or dryness (which is more common if your ovaries have been removed at the time of the hysterectomy) you may wish to try a vaginal lubricant. You can buy this from your local pharmacy.
Following a laparotomy the rate of recovery depends on each individual and to a large extent on your state of health before the operation. It is important that you resume your normal activities gradually and limit what you do by how tired or uncomfortable you feel.
Continue with any exercises that you were advised to do in hospital. You may find that you get tired quite quickly at first. This is normal and will improve along with your general fitness level.
Returning to work is up to the individual concerned and depends on the type of job you do. Any job requiring heavy lifting may take a bit longer to return to, usually about 12 weeks, but if you are in a job with no lifting involved, you may be able to return after six to eight weeks but you are the best judge as to how you feel.
Remember, however, that you have had a major operation and time is needed to allow the healing of the wounds.
You can normally resume driving when you can stamp your feet hard on the ground without causing pain or discomfort, and when you believe that your concentration will not be impaired. Your insurance company will probably assume that you are not fit to drive after a major operation until your doctor says you can. If you have any concerns about this, check with your own GP.
General advice
If you have any of the following symptoms, you should contact your GP:
- A smelly vaginal discharge or bleeding which is heavy and ‘fresh’ (bright red) or the passing of clots
- Pain which is severe and not controlled by your prescribed painkillers
- Feeling unwell, hot and feverish
- Pain in the calf muscles or chest
- Signs of a chest, wound, urine or vaginal infection.
Breathing exercises
The recommended breathing exercises mentioned should help maintain a clear chest, tone up muscles and ease wind pain following surgery. Start this exercise as soon as you wake up from the anaesthetic and do regularly until you increase your walking.
Bend your knees up with feet flat on the bed, breathe in through your nose until your lungs are as full as possible, then relax as you breathe out through your mouth. Repeat five times every half hour or so, and follow with two huffs.
Huff: Position as above with hands or pillows supporting any area of discomfort. Take a medium breath in, then force the air out quickly through an open mouth, as though you are trying to mist up a large mirror. Follow this with a cough – take a big breath in first, and do not worry about this doing any damage in the area of your surgery.
Foot and knee exercises
These should help the circulation and help prevent clots from forming in your legs. Repeat every time you do your breathing exercises and until you are walking about. Bend feet up and down at the ankle firmly and quickly. Draw circles with your feet. Press back of the knees into the bed and tighten up the thigh muscles.
We hope you have found this information helpful.
Ova the rainbow

Ova The Rainbow is a support group for anyone who would like support for themselves or their friends and family due to any gynaecological cancer.
It was established at the end of 2001 by two specialist oncology nurses, Jane McNeil and Lynne Wright out of The James Cook University Hospital. The Friarage branch was established in 2005 by Maggie Wright.
We are a registered charity and our meetings are held monthly for friends, family and any other supporters.
First Tuesday of the month, 2pm to 3:30pm
Allerton Court Hotel, Darlington Road, Northallerton, North Yorkshire DL6 2XF
For further details please contact: 01642 282418
Contact information:
- Appointments Desk:
01642 854861
01642 282714
01642 854883 - Gynaecology outpatients department (including pre-admission service): 01642 854243
- Surgical admissions unit: 01642 854603
- Ward 8: 01642 854508
- Gynae oncology nurses (Monday – Friday 8.30am-5pm): 01642 282418
Further information
- Visit the macmillan website
- Visit the cancer research website
- The Royal College of Obstetricians and Gynaecologists,
27 Sussex Place, London NW1 4RG.
More patient information is available on the RCOG website:
Patient experience
South Tees Hospitals NHS Foundation Trust would like your feedback. If you wish to share your experience about your care and treatment or on behalf of a patient, please contact The Patient Experience Department who will advise you on how best to do this.
This service is based at The James Cook University Hospital but also covers the Friarage Hospital in Northallerton, our community hospitals and community health services.
To ensure we meet your communication needs please inform the Patient Experience Department of any special requirements, for example; braille or large print.
T: 01642 835964
E: [email protected]