Physiotherapy
Below you will find some important information about your shoulder stabilisation surgery and subsequent recovery. The instructions and exercises provided are given as a guideline only. Each patient is treated as an individual and the care you receive may vary slightly.
If you are in any doubt or have any questions about the information provided please ask a member of the shoulder team.
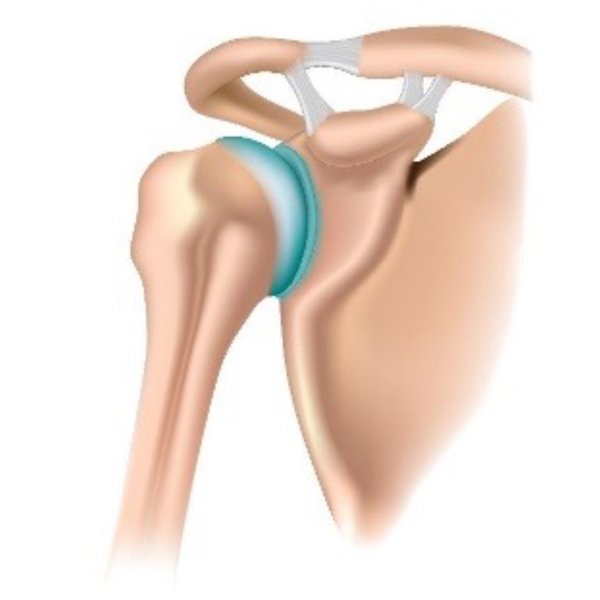
The shoulder joint
The shoulder is the most mobile joint in the human body. It is formed between the ball shape at the end of the upper arm bone (humeral head) and a nearly flat surface of the shoulder blade that forms the socket (glenoid).
The joint relies on the muscles around the ball and socket (the rotator cuff), a rim of cartilage on the glenoid (the labrum) and surrounding ligaments to maintain its stability.
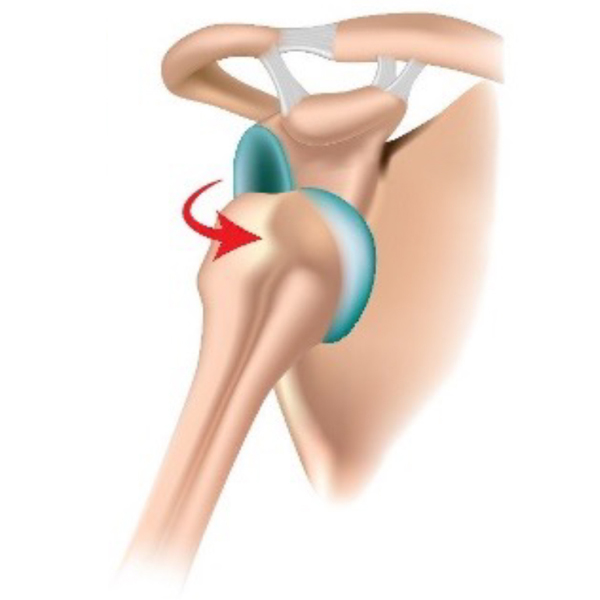
What is shoulder instability?
Shoulder instability commonly develops following a separation (dislocation) of the bony surfaces (humeral head away from the glenoid). Most shoulders will dislocate forwards and/or downwards. Approximately only 10% of dislocations are backwards.
Shoulder dislocation
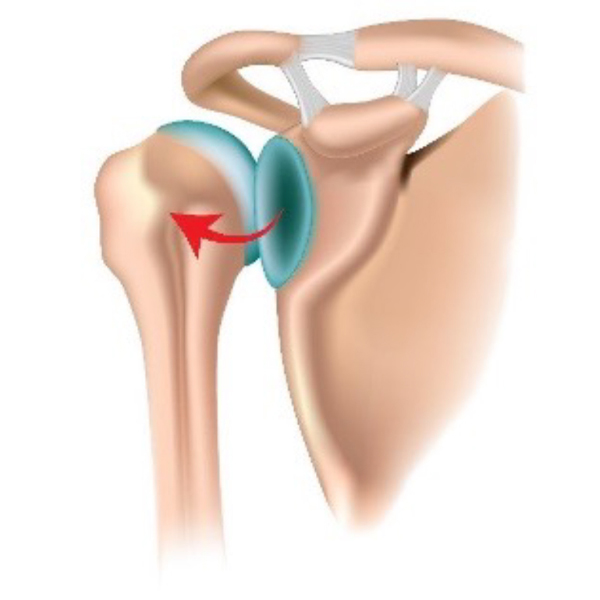
Dislocations are more common in younger patients and are often a result of injury, such as when playing contact sports. This can result in the labrum being separated from the bone at various points. The ligaments can also become stretched or torn. Injury to these structures surrounding the joint can result in the shoulder becoming unstable.
Symptoms of instability can include; pain, reduced movement due the shoulder feeling unstable and repeated dislocations or ‘subluxations’ (partial separation of the joint surfaces).
It is hoped that by surgically stabilising the shoulder these symptoms will resolve helping you return to your work and usual activities.
The treatment for shoulder instability following one or more previous dislocations can depend on your age at the time of your first dislocation. Younger patients (under the age of 25) are more likely to require surgical stabilisation of the shoulder, whereas older patients may be able to manage their instability with physiotherapy.
What is shoulder stabilisation surgery?
The surgery is carried out under a general anaesthetic and once you are asleep your surgeon will examine your shoulder joint, determining the direction and extent of instability in your shoulder. They will use key holes to insert a small ‘telescope’ and camera into your shoulder (this procedure is known as ‘arthroscopy’) to carefully look and identify what injury has occurred.
There are two main types of stabilisation surgery that may be performed by your surgeon. A member of the surgical team will be able to discuss the type of surgery that you may require.
- Bankart repair:
This is a soft tissue repair that involves reattachment and tightening of the torn labrum and ligaments of the shoulder. The procedure is usually done through ‘key holes’, but rarely may need to be done as an ‘open’ operation with a larger scar. - Laterjet procedure:
This is performed when there has been an injury to the bone at the front of the socket (glenoid); a piece of bone from elsewhere is fixed to the front of the socket to re-build the front of the socket where the bone has been damaged. This is usually done as an ‘open’ operation.
What are the potential risks?
Although rare, all operations have some potential risks or complications and it is important that you are aware of them.
Minor side effects such as sickness and nausea, sore throat and discomfort are relatively common, and you may need medication to help control such symptoms.
More serious complications such as allergies, chest infections, dental damage and nerve damage are rare.
Important
If you have a known allergy to any medication it is important that you make your anaesthetist aware.
Complications such as upsetting the heart, lung, kidney or brain function are even rarer.
General surgical risks:
- Blood clot or DVT
You are more at risk of developing deep vein thrombosis following an operation. These risks are similar to those potentially encountered on a long haul flight. - Infection
Some people may develop a minor infection, which may need treatment with antibiotics. Occasionally more serious infections may occur in the shoulder joint after the operation. This may require further surgery and treatment with antibiotics. The risk of infection is low, generally under 1%. - Warning Signs:
Following your operation, if you develop a high temperature, become unwell, notices pus in your wound and, or your wound becomes red, sore or painful, please contact a member of your surgeon’s team immediately. If you are unable to contact the surgical team, please attend the Emergency Department immediately. - Recurrent instability:
Although rare sometimes the repair can fail and result in further instability of the shoulder, this may require further surgery. - Persistent pain and, or stiffness in the shoulder:
It is possible that some pain may remain in the shoulder following surgery and that you do not regain your full movement, however this should not limit your ability to use the shoulder.
What happens on the day of your surgery?
On the morning of your surgery you will be assessed by a member of the surgical team and an anaesthetist to confirm that you are ready for surgery. They will also answer any questions that you may have about your surgery. You will also be required to sign a form giving your consent to proceed with the operation if you have not done so already.
Important
It is important that you do not have anything to eat (even chewing gum) in the 6 hours prior to your operation. You may drink clear fluids up until 2 hours before your operation. Eating or drinking, anything closer to your operation may result in the surgery being delayed or cancelled.
Anterior shoulder stabilisation surgery is usually performed under a general anaesthetic.
An injection of local anaesthetic around the nerves in the neck that supply the arm called an ‘interscalene nerve block’ may be used in your shoulder surgery. This is usually performed by the anaesthetist with the guidance of an ultrasound machine to identify the correct nerves and minimise risk. This nerve block is often used, as it provides a good form of pain relief for the first 24 hours after the operation.
If you have had a nerve block, your arm will feel numb and heavy but this should resolve within 24 hours.
Following your surgery you will be taken to recovery before being transferred to the Day Surgery Unit. Your arm will be placed in a sling and there will be a dressing over your surgical sites.
Once you have recovered sufficiently from your anaesthetic you will be seen by a physiotherapist who will give you advice about wearing your sling. They will also teach you some exercises, which you can begin once your nerve block has worn off. The majority of people can go home on the same day of their surgery but occasionally it may be necessary to stay overnight.
The physiotherapist will also arrange an outpatient physiotherapy appointment for you to continue with your rehabilitation.
What happens after your surgery?
You will be expected to perform your exercises at home, as advised by your physiotherapist and continue taking regular pain relief tablets. You will normally have to visit your GP Practice ten days following your surgery to have your wound checked and if stitches have been used, they will be removed.
You will be referred for outpatient physiotherapy to continue with your rehabilitation and this will normally start one to two weeks following your surgery. If you have any questions or concerns before this time, please do not hesitate to contact a member of the shoulder team.
Gaining the best outcome following your surgery takes time and rehabilitation. You are likely to see most of the improvement in the first three to six months following your surgery, but sometimes a more gradual improvement can continue for between one and two years.
You will have a review appointment in a post-operative shoulder clinic between four and six weeks after your surgery. This appointment will be with a member of the consultant’s team or an advanced physiotherapy practitioner.
General advice
Pain control
It is normal to have some pain and discomfort in your shoulder following your stabilisation surgery. It is recommended you take regular pain relief as advised by the hospital team to help keep this under control. Keeping your pain well controlled will help with your recovery. If you feel that you require any further medication then please visit your General Practitioner (GP).
Once your sensation has returned around your shoulder you can use ice to help with managing your pain. To apply ice, wrap an ice pack or bag of frozen peas in a damp towel and then place the ice on your shoulder for 10 to 15 minutes, 3 to 5 times a day. It is important to never apply ice directly to your skin. You can wrap your ice pack in a plastic bag or wrap it in cling film to keep your dressings dry.
Be aware of the position of your shoulders if you are getting pain. If you feel tense, try taking a deep breath in, and then, when you breathe out letting your shoulders relax. Being aware of your breathing may also help to reduce tension, as it is easy to hold your breath or forget to breathe correctly when you are in pain.
Wearing your sling
You will normally have to wear your sling for four weeks after the surgery. This will not only help to protect the stabilisation and allow healing, it may also help with pain relief. You can remove your sling to perform your exercises and when washing and dressing. You can use your hand for very light tasks for example, reading or using a computer whilst your arm is supported in the sling, but there should be no pain in your shoulder as a result.
Do not try to use your arm for daily activities out of the sling. You should not lift your arm away from your body on its own, reach behind your back or carry anything with your operated arm until advised to do so by your physiotherapist.
Before you go home, a physiotherapist will show you how to take your sling on and off and how to look after your arm when using the sling.
Sleeping

Initially you may find it more comfortable to sleep in a more upright position supported by pillows.
Placing a pillow underneath your arm may support the arm when lying down.
Do not sleep on your operated side for the first six weeks and after this be guided by how comfortable your shoulder feels. Initially you will need to wear your sling when sleeping to support your shoulder.
Washing and dressing
You can usually wear your sling over indoor clothing but underneath bulky outdoor clothing. You might find it easier to wear loose fitting clothing that buttons down the front. When washing and dressing try to keep your operated arm as still and relaxed as possible. Try to keep your sling as clean and dry as possible (you should ask for a replacement sling if yours becomes dirty or uncomfortable).
Remove your sling by sitting with your arm supported on a pillow. Undo the velcro fastenings at the elbow and the wrist and gently slide the sling out. First, thread your sleeve onto your operated arm and take the item of clothing up to the shoulder as far as possible. Next, place your non-operated arm into the other sleeve bringing the garment up and around your shoulders and fasten the clothing.
Replace the sling by gently sliding it under your forearm and securing the velcro fastening (you may need to lean forward and support your arm on the table to help with this). For undressing perform the routine in reverse.
It is important to wash your elbow creases and underneath your arm pit to prevent any soreness whilst in the sling. To do this sit at a table with your arm supported on a pillow. This will allow you to comfortably wash under your arm.
Domestic tasks
It may be useful to prepare meals in advance prior to your surgery or have meals that require little preparation, for example, pre chopped vegetables. You should avoid heavy household tasks for at least twelve weeks after your surgery, but you can begin gentle daily activities once you come out of your sling. Your physiotherapist will be able to guide you further with regards to returning to these activities.
Driving
You will be unable to drive whilst you are in your sling. Return to driving is normally six to eight weeks following your surgery. Your physiotherapist will help guide you on when you have sufficient movement and a good level of pain control to be able to drive.
Your physiotherapist will help guide you on when you have sufficient movement and a good level of pain control to be able to drive. You need to make sure that you have full control of the vehicle and are able to perform an emergency manoeuvre if needed. It is a good idea to start with a short journey and build up slowly.
Work
You will normally be off work for between four and twelve weeks depending on the type of work that you do. It is advised not to perform any heavy lifting, overhead or manual work for four to six months following your surgery. If you have any queries regarding this please discuss with your consultant or physiotherapist.
What to avoid after your surgery?
- Lying on your operated arm following your surgery for the first six weeks (this will likely be very uncomfortable)
- Reaching behind your back or behind your head, with your operated arm
- Lifting or carrying anything with your operated arm until advised to do so
- Driving (you will be advised when it will be safe to start driving)
- Operating machinery whilst wearing the sling
Physiotherapy
Physiotherapy will form an important part of your recovery following your stabilisation surgery. Once you can come out of your sling the aim is to regain movement in your shoulder and start using your arm for light daily activities. When you have regained good movement and control of your shoulder you will then begin working on increasing the strength and endurance of the muscles surrounding your shoulder. This will then progress to more specific rehabilitation depending on your individual goals.
The physiotherapist on the ward will teach you some exercises that you can begin once your nerve block has worn off. Initially following your surgery, the aim is to protect the stabilisation whilst it starts to heal. It is important to start moving the shoulder soon after surgery to prevent stiffness. It is normal to have some mild discomfort and pulling in the shoulder with your exercises, but they should not cause pain.
It is important not to force or stretch your shoulder initially. The exercises may vary slightly depending on any specific instructions that have been given by your consultant. Try to keep active after your surgery, taking regular walks can help with your recovery.
Neck exercises
It is important to keep your neck moving as it can become stiff when wearing the sling. Move your neck in all directions, look up, look down, and turn to the right and to the left regularly through the day.




Elbow, wrist and hand exercises
Make an effort to keep your wrist and fingers moving every couple of hours whilst you are wearing your sling, to prevent stiffness and to maintain your circulation. Move your wrist up and down and draw circles. Try to keep your fingers moving by opening and closing your hand regularly.
To prevent any stiffness in your elbow it is important to perform a few exercises when you remove your sling.




With your elbow bent and tucked into your side turn your palm up to the ceiling and down towards the floor.
Bend your elbow bringing your hand towards your shoulder and then straighten your elbow as far as you can, you can support the forearm with your non operated arm initially if this is more comfortable.
Shoulder exercises
Postural exercises
In sitting, slump down into your seat rounding your shoulders, then sit up tall squeezing your shoulder blades together. Then slowly shrug your shoulders up to your ear and roll your shoulders back down.



up to your ears

Supported flexion
Place your hands hands flat on a table. Place a towel underneath your hands and gently slide the arms forward on the table using the non-operated arm to assist. Slide the arms away from the body as far as comfortable before bringing the arms back in towards your body. This exercise can be performed in sitting or standing.


and gently slide the arms forward
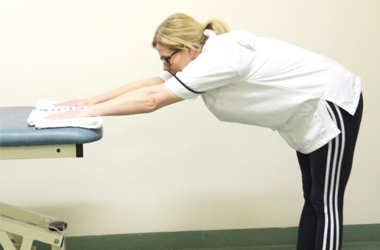
Walk away
Stand in front of a table with your palms placed flat on a table. Slowly walk your feet away from the table as far as you feel comfortable. You do not need to force or stretch this movement. Stay in this position for 5 seconds before walking your feet back to the starting position.

Outward rotation
Your physiotherapist will advise you how far you can perform this exercise initially. This helps to prevent stiffness from wearing the sling. It is normal for this movement to feel stiff following your surgery. It is important not to force or stretch this movement in the first four weeks.
You can perform this exercise sitting or standing. Holding a walking stick (or something similar) in both hands, gently move your operated arm out to the side and then back
to your starting position. Keep your elbows tucked into your side during this exercise, placing a towel between your elbow and side can help with this.


If you experience any of the following:
- A change or worsening of your pain
- Increasing redness, swelling or oozing around the wound
- Loss of sensation in your arm
- A sudden loss of movement in your operated arm
- Prolonged tingling or pins and needles in the arm
- Fingers or hand turning cold and clammy or blue
Then please let your physiotherapist know or contact a member of the upper limb team as soon as possible.
Contact us
Contact the physiotherapy department on:
Telephone: 01642 854453
Email: [email protected]
Patient experience
South Tees Hospitals NHS Foundation Trust would like your feedback. If you wish to share your experience about your care and treatment or on behalf of a patient, please contact The Patient Experience Department who will advise you on how best to do this.
This service is based at The James Cook University Hospital but also covers the Friarage Hospital in Northallerton, our community hospitals and community health services.
To ensure we meet your communication needs please inform the Patient Experience Department of any special requirements, for example; braille or large print.
T: 01642 835964
E: [email protected]