
Spinal Cord Injuries
What does the procedure involve?
Placement of drainage tube into bladder through an incision in the skin over the bladder area (just above the pubic hairline). Cystoscopy (inspection of the bladder) is often performed to aid insertion of this tube.
What are the alternatives to this procedure?
Alternatives to this procedure include a catheter through the urethra and permanent urinary diversion.
What should I expect before the procedure?
You will usually be admitted to hospital the day before for your surgery. Once you have been admitted, you will be seen by a member of the urology team.
Immediately before the operation, the anaesthetist may give you a pre-medication which will make you dry-mouthed and pleasantly sleepy.
Please tell your surgeon (before your surgery) if you have any of the following:
- An artificial heart valve
- A coronary artery stent
- A heart pacemaker or defibrillator
- An artificial joint
- An artificial blood-vessel graft
- A neurosurgical shunt
- Any other implanted foreign body
- A regular prescription for warfarin, aspirin or clopidogrel
- A previous or current MRSA infection
- A high risk of variant-CJD (if you have had a corneal transplant, a neurosurgical dural transplant or injections of human-derived growth hormone)
When you are admitted to hospital, you will be asked to sign your operation consent form giving permission for your operation to take place, showing you understand what is to be done and confirming that you want to go ahead.
What happens during the procedure?
Either a full general anaesthetic (where you will be asleep) or a spinal anaesthetic (where you are unable to feel anything from the waist down) will be used. All methods reduce the level of pain afterwards.
You will usually be given injectable antibiotics before the procedure, after checking for any allergies.
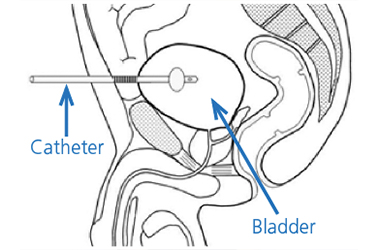
The surgeon will first fill your bladder with fluid and then insert your suprapubic through a small incision in your lower tummy (pictured), just above the pubic hairline.
In patients with small bladders, the incision Bladder often needs to be larger so that the bladder can be seen clearly to allow the catheter to be inserted. Correct positioning within the bladder is checked by telescopic inspection of the bladder via the water pipe (urethra).
What happens immediately after the procedure?
You should be told how the procedure went and you should:
Ask the surgeon if it went as planned
Let the medical staff know if you are in any discomfort
Ask what you can and cannot do
Feel free to ask any questions or discuss any concerns with the ward staff and members of the surgical team
Make sure that you are clear about what has been done and what happens next
The catheter may be stitched in place at first, but these stitches can be removed after a week or so, without the catheter falling out. The average hospital stay is two days.
Are there any side-effects?
Most procedures have possible side-effects. But although the complications listed below are well-recognised, most patients do not suffer any problems.
Common (greater than 1 in 10)
- Temporary mild burning or bleeding during urination.
Occasional (between 1 in 10 and 1 in 50)
- Infection of the bladder needing antibiotics (occasionally, recurrent infections)
- Blocking of the catheter needing unblocking
- Bladder discomfort and pain
- Persistent leakage from the water pipe (urethra) which may need a further operation to close the bladder neck
- Development of stones and debris in the bladder, causing catheter blockage, and requiring removal or crushing by a further procedure.
Rare (less than 1 in 50)
- Bleeding requiring irrigation, or additional catheterisation, to remove blood clot
- Rarely, damage to surrounding structures, such as bowel or blood vessels with serious consequences, possibly needing additional surgery.
Hospital-acquired infection
- Colonisation with MRSA (0.9% – 1 in 110)
- MRSA bloodstream infection (0.02% – 1 in 5000)
- Clostridium difficile bowel infection (0.01% – 1 in 10,000)
The rates for hospital-acquired infection may be greater in high-risk patients, for example those patients
- with long-term drainage tubes;
- who have had their bladder removed due to cancer;
- who have had a long stay in hospital; or
- who have been admitted to hospital many times.
What should I expect when I get home?
When you are discharged from hospital, you should:
- Be given advice about your recovery at home
- Ask when you can begin normal activities again, such as work, exercise, driving, and housework
- Ask for a contact number if you have any concerns once you return home
- Ask when your follow-up will be and who will do this (the hospital or your GP)
- Be sure that you know when you get the results of any tests done on tissues or organs that have been removed.
When you leave hospital, you will be given a ‘draft’ discharge summary. This contains important information about your stay in hospital and your operation. If you need to call your GP or if you need to go to another hospital, please take this summary with you so the staff can see the details of your treatment.
This is important if you need to consult another doctor within a few days of being discharged.
The catheter will need to be changed, for the first time, after approximately six weeks and we will arrange this for you in the outpatient clinic. Thereafter, further catheter changes can be performed by your GP or district nurse.
The safe use of a leg bag
Leg bags are usually attached either to your thigh or to your calf with a pair of straps. Alternatively, the leg bag may be worn inside a special sock against your leg. How you wear your leg bag depends on what feels comfortable.
What happens when the leg bag fills up?
As the leg bag fills, it gradually gets heavier and you will feel a strain on the straps. It is best not to let your leg bag get too full.
To empty, open the tap at the bottom and let it drain – into the toilet, if possible. If you find this difficult, you can use a container, but you must keep it for this purpose only. Do not forget to close the tap again after you have emptied the leg bag, and always wash your hands.
What happens at night?
When you go to bed your leg bag should be connected to a bed bag. This is larger and can hold more urine, so that you do not have to get up at night to empty the bag.
- Loosen your leg straps when you get into bed
- The bed bag must not be allowed to lie on the floor
- Support it on a special hanger or stand
What else should I look out for?
- If you develop a fever, redness in the wound, any pus from the catheter site or worsening bleeding, you should contact your GP immediately.
- In the event of the catheter falling out, it must be replaced as a matter of urgency or the track will close up and it may not be possible to re-insert the catheter. Contact your GP for immediate advice or come directly to your local Accident & Emergency Department.
Are there any other important points?
Some discharge from the catheter site is not unusual in the longer term. If the catheter blocks within the first four weeks, the channel between the skin and the bladder will not have healed completely so it is not possible to change the catheter easily.
In this event, it is important that the catheter is not taken out in an attempt to change it. It should simply be left in place and a urethral catheter inserted as well, followed by immediate notification of the urology specialist nurse.
Patient experience
South Tees Hospitals NHS Foundation Trust would like your feedback. If you wish to share your experience about your care and treatment or on behalf of a patient, please contact The Patient Experience Department who will advise you on how best to do this.
This service is based at The James Cook University Hospital but also covers the Friarage Hospital in Northallerton, our community hospitals and community health services.
To ensure we meet your communication needs please inform the Patient Experience Department of any special requirements, for example; braille or large print.
T: 01642 835964
E: [email protected]