Cardiothoracics
This information booklet has been prepared to help you and your relatives understand more about your heart operation. It aims to provide you with general information about what to expect from the time you are accepted for surgery, when you are admitted to hospital and through to your discharge home from James Cook University Hospital.
The Enhanced Recovery After Surgery (ERAS) programme is aimed at helping you prepare for and recover from major surgery as effectively as possible. It can maximise your chances of a speedy recovery and minimise your hospital stay. We believe that your support network (friends, family, partner etc) are central to your recovery.
What is an enhanced recovery programme?
Enhanced recovery is a modern, evidence-based approach that helps patients who are undergoing surgery to recover more quickly.
Different members of the hospital and primary care team work together in order to ensure patients are:
As healthy as possible before receiving treatment
Receive the best possible care during their operation
Receive the best possible care while recovering
How does it work?
We are committed to managing your care based on your individual needs during and after your operation.
We aim to:
- Reduce pain with anaesthetic techniques and medication to suit you
- Support and encourage early movement and activity
- Remove drips, drains and catheters as early as possible
- Reduce post operative nausea and vomiting by managing your fluid balance and with medication.
Common types of cardiac surgery
Coronary artery bypass grafts and heart valve repair or replacements are the most frequent heart operations performed at James Cook Hospital. However, for some people it will be necessary to perform other types of cardiac surgery.
Coronary artery bypass grafting (CABG)
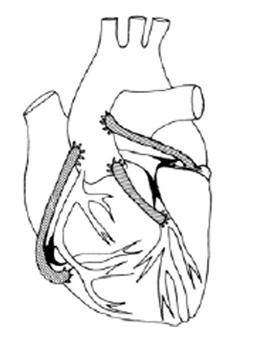
You will have had an angiogram which will have shown that you have a narrowing (stenosis) in one or more of your coronary arteries. The surgery required for this type of heart disease is known as Coronary Artery Bypass Grafting, or CABG.
This operation involves the joining of a blood vessel onto the heart to bypass the narrowed coronary artery – we term this as a graft or grafting. (See diagram)
Usually veins from the legs or occasionally an artery from the arm can be removed and used as the new graft. The artery running down behind the chest wall, called the internal mammary artery, is frequently used in a similar way.
Heart valve repair or replacement
The heart has four one way valves to help the flow of blood around the body and lungs. You may have had a scan of your heart called an “echo” which is used to look at how the heart pumps and can identify leaky (regurgitation) or narrowed (stenosed) heart valves. The normal flow of blood through the heart can be prevented if these problems exist.
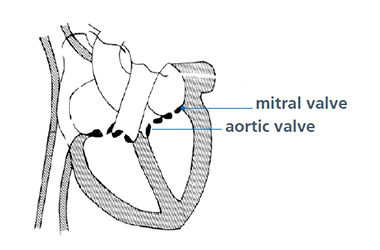
The two most commonly affected valves are called the mitral and aortic valves. The aortic valve is generally replaced whereas the mitral valve can sometimes be repaired rather than replaced. Should a repair not be possible and a replacement is required, you will receive an artificial heart valve. This will either be made of mechanical parts or of natural tissue. (See diagram).
Types of valve: mechanical and tissue
When you see the cardiac surgeon, they will discuss the advantages and disadvantages of both mechanical and tissue valves. Although the surgeon may advise which they feel is the best type of valve for you, the final choice will be yours.
Mechanical valves
The advantage of having a mechanical valve is that they are more hard wearing than tissue valves. Thereby, avoiding the need to have further surgery in the future.
You may initially be aware of your valve making a quiet ticking noise similar to the sound of a ticking watch, especially when the surrounding environment is quiet. This will become natural to you and your family. It is normal for the valve to do this.
The disadvantage of having a mechanical valve is that you will have to be on a tablet called Warfarin for the rest of your life.
Warfarin
Warfarin is a tablet that thins your blood in order to prevent it clotting around the mechanical valve. When taking Warfarin you are required to have regular blood tests to make sure that your blood is not too thick or too thin.
This blood test is known as the International Normalised Ratio (INR), and before you go home from hospital the Doctor will give you a target INR range to keep your clotting levels safe for you.
Your GP or local hospital will continue to monitor your INR levels and will instruct you on the dose of Warfarin you will need to take and how often you will need to have blood tests.
Important
Warfarin MUST NOT be stopped without medical advice.
Tissue valves
The tissue valves used at James Cook Hospital are made from either porcine (pig) or bovine (cow) tissue. The major advantage of having a valve made of tissue is that you do not need to take Warfarin after your surgery.
At present we know that these valves last approximately ten to 15 years depending on your age. If you choose a tissue valve you may need a further operation in the future to replace it if it wears out.
Cardiac outpatients or in-house
If you have been referred by a cardiologist and have attended the outpatient department to meet with a cardiac surgeon, you are known as an elective patient. These patients wait at home and are booked to come in for their surgery.
If you have been admitted to hospital because you require urgent cardiac surgery, you are known as an ‘in-house urgent’ patient. This group of patients wait for their surgery either in their local district hospital or in James Cook Hospital.
Pre-assessment clinic
Elective patients will be seen in the cardiothoracic outpatient department. At this appointment you will meet several members of the surgical team.
You will be seen by the consultant cardiac surgeon who will discuss the indications, along with the risks and benefits for your proposed surgery. The surgeon will also discuss if any alternative procedures available with its risks and benefits. If you are happy to proceed, you may be asked to sign a consent form at this time.
The cardiac anaesthetist will assess your anaesthetic requirements and plan the necessary care, talk to you about our methods for controlling postoperative pain, inform you of when to stop eating and drinking prior to your surgery and they may ask you to withhold or reduce the doses of some of your medications on the day of surgery and they may ask you to withhold or reduce the doses of some of your medications on the day of surgery.
The cardiac specialist nurse or surgical care practitioner (SpN or SCP) will carry out the preassessment for your surgery.
The SpN or SCP will take a detailed medical history, go through your current medications with you and carry out a physical examination.
You will meet one of the nurses from our ward 32 who will complete a nursing assessment, take your blood pressure, pulse and oxygen levels. The nurse will also take some blood tests, a nasal and groin swab, they will perform an electrocardiograph (ECG) and send you for a chest xray.
Prior to leaving the pre-assessment clinic you will be provided with a prescription for an antibacterial body wash and antibacterial nasal ointment that should be collected at James Cook outpatient pharmacy. This wash and nasal cream are to help reduce the risk of wound infections after your surgery.
You should start to use this treatment 5 days before your admission day
Where appropriate you will be given some carbohydrate drinks to take on the evening before and the morning of your operation. These drinks provide you with extra carbohydrates and help prepare your body for surgery.
Getting ready for surgery
Knowing about your risk factors, how they affect your health and how they increase your risk may help you to make lifestyle changes and can help you to feel more in control of your health. You can access more information on the subject in the Cardiac Enhanced recovery through the South Tees Hospital website.
James Cook University Hospital runs a number of research projects. We would be grateful if you could participate in one of our on-going studies. Please let one of the members of the team know of your interest and we will explain to you in more detail.
Lifestyle
There are certain risk factors that can contribute to heart disease, particularly coronary heart disease. Once you have been referred for heart surgery, use the waiting time to raise your overall level of fitness.
There are 5 main things you can do:
- Keep physically active
Although some people waiting for surgery may be limited in the amount of activity they can do, gentle exercise can help keep you moving and as fit as possible.
Discuss with your nurse or doctor the amount of activity that you can safely do. However, if you get chest pain during exercise you should stop and rest before continuing providing it settles completely.
- Stress
Waiting for heart surgery can be stressful. Some people may believe that stress played a part in the development of their heart problem.
Events leading up to the illness may have accelerated the process, but it is important to be clear that heart disease is a chronic disease of the coronary arteries and any damage to the tissues and, or valves will have taken place over time.
Stress however can have a significant influence on the rate of recovery and your confidence to return to your normal lifestyle. Stress can raise your blood pressure which is ideally best avoided before surgery.
It is important to address any concerns or questions you may have to avoid a build up or fear of uncertainty. - Diet
Diet can affect your heart health in many ways. This will be explained in more detail in the “post-op information” section.
Before cardiac surgery, the most important dietary messages are:
• Drink plenty fluids
• Eat regular meals
• Follow a balanced diet; a wide range of foods, including fruit and vegetables, starchy foods, dairy foods and meat and fish or alternatives
Ideally, in the weeks leading up to surgery, you should be well nourished, to help you to recover faster following the operation. If you have experienced any unintentional or rapid weight loss recently, or a loss of appetite, please alert your family doctor who may refer you to a Dietitian.
When you arrive on the ward you may notice they have different menus to the general wards; these are based on healthy heart guidelines. - Smoking and alcohol
If you smoke, it would be better if you tried to stop smoking.
Smoking makes the coronary arteries narrower and encourages blockages in them. It also damages your lungs. If you continue to smoke right up to the time of operation, it may increase the risk of complications after the operation such as breathing problems and may also affect the healing of your wounds.
If you drink a lot of alcohol we recommend that you reduce the amount that you drink prior to your surgery. Alcohol can reduce the function of your heart and it also causes mild dehydration. However, reducing high alcohol intake suddenly when you come into hospital can also cause serious health problems, so it is better to cut down well in advance.
If you need help to stop smoking and alcohol, ask your doctor or local pharmacist about counselling or nicotine replacement products.
- Breathing exercises
Chest problems can occur after surgery even if you have no history of chest illness or smoking. The physiotherapist will give you exercises before the operation to keep your lungs clear of phlegm and make sure your lungs are opening up well.
Several breathing exercises are recommended to help reduce the likelihood of chest problems after your operation.
Please start practicing these by yourself as soon as possible before your operation to help develop a routine.
- Sit upright with your hands placed over the sides of your chest.
- Take a deep breath in slowly through your nose.
- Hold this breath in for one to two seconds and then.
- Breathe the air out slowly through your mouth.
- Repeat 5 times, then huff 5 times.
To do a huff, take a medium sized breath in then force the air out quickly through an open mouth, as if you are steaming up a window or glass.
Your hospital stay – what to expect
When will I be admitted?
Sometime after your pre-assessment clinic appointment, your consultant surgeon’s secretary will advise you on when you will be admitted to hospital for your surgery.
Normally if you are having your operation in the morning, you will be admitted to our department the night before your surgery.
If you are having your operation in the afternoon, then you will be admitted that morning.
What do I need to bring in?
We advise you to bring in a minimal amount of personal belongings with you. This is a guide to what you may need whilst you are in hospital
The tablets that you are currently taking.
You will be provided with a green pharmacy bag when you attend the pre-assessment clinic to put all of your medicines in, ideally your medicines will be in their original packaging.Nightwear x3
Toiletries
Sturdy slippers or shoes
To avoid slips and falls, sturdy slippers or shoes should be worn at all times when standing or walkingDressing gown
Loose change
Any walking aids that you use
Please avoid bringing in the following
Items of value, including sentimental value
Bank cards and cheque book
Excessive amount of money
Day of admission
You will be admitted to either our cardiology admissions day unit (CADU) or ward 32 prior to your operation.
Before the operation you will be visited by a number of staff, including the anaesthetist and surgeon who will recap on the information you have already received regarding your surgery and give you a chance to ask any questions you may have.
If not already completed at your pre-assessment clinic appointment, you may be asked to sign your consent form at this point.
Important
Before your operation, the following preparation will be required
Bath or shower
It is important for any patient having surgery that the skin is as clean as possible in order to reduce the risk of infection. Ward staff will advise you to have a bath or shower and wash your hair using an antiseptic soap the evening before and the morning of the surgery. If you are too unwell to have a bath or shower, the nurse will help you at the bed side.
Eating before your operation
The ward nurse will keep you informed as to when you must stop eating and drinking (nil by mouth). Normally it is 6 hours fasting for solid food and 2 hours for clear fluid before surgery
The pre-med
Normally one or two hours before your operation you will be given a pre med. We give an antacid tablet called Lansoprazole before taking you to theatre. If appropriate you will also be asked to have a further carbohydrate drink prior to your surgery.
Going into theatre
When the theatre staff are ready you will be taken to the operating theatre on a trolley. A healthcare assistant (HCA) form theatre and a ward nurse will accompany you.
Once in the anaesthetic room, the anaesthetist will check your identity with you, your name bands and your medical notes and put a couple of drips into your arm (one in your vein and one in your artery). You will be given some oxygen through a facemask for few minutes, you will receive an injection of drugs into your vein and you will then be asleep for the whole operation.
You will be in the operating theatre for 3 to 6 hours, but this is just a guide. Some patients are in theatre for shorter or for longer, depending on what kind of operation is being performed. After your operation you will be transferred to the Cardiac Intensive Care Unit.
During your operation a number of other tubes, lines and drains will be inserted, while you are asleep, which you will be aware of when you wake up.
These include:
- A drip in a vein (central line) in the side of your neck to monitor your vital signs and give you medications and fluids.
- Chest drains at the base of your chest wound to drain any excess blood left from the operation
- A small tube in your bladder to drain your urine, called a urinary catheter.
- Temporary pacing wires
Cardiac surgery ward round
What to expect during ward rounds
Daily Visits
- The Cardiac care team will visit you to review your progress daily.
- They may adjust treatments, and plan the next steps in your care.
Questions and Updates
- Ward rounds are a great time to ask questions and receive updates about your treatment plan.
- Feel free to discuss any concerns you have about your recovery.
Review and Planning
- The team will review your medical charts, discuss their observations with each other, and make decisions about your ongoing treatment.
- This collaborative approach ensures that you receive comprehensive care tailored to your needs.
Family Involvement
- If you wish, family members can be present during ward rounds to help understand your condition and treatment plans.
- Please inform your nurse or doctor if you want your family to be involved.
General information
- Ward rounds usually take place in the morning, on weekdays.
- This may be later during weekends, or if there is an emergency.
- The core cardiac surgical ward round team may have:
- a Specialty Registrar (SpR) and
- an Advanced Nurse Practitioner (ANP), Surgical Care Practitioner (SCP) or Senior House Officer (SHO)
- You may also come across some of the other team members mentioned in this leaflet. (see below for role details)
- There may be 1 to 6 people present on the ward round team, depending on your phase of recovery.
- The consultants may come to see you separate to this ward round.
Please note: this may not be daily and will be as and when required depending on your stage in recovery.
Meet your cardiac ward round team

- Consultant Cardiac Surgeon
- Role: leads the surgical team, performs surgery, and makes key decisions about your care.
- Responsibilities: assessing your condition, discussing treatment options, overseeing surgical procedures, and managing your care after the operation.

- Specialty Registrar (SpR)
- Role: a doctor training in Cardiothoracic surgery.
- Responsibilities: assists in surgeries and leads morning ward rounds. Please note – may wear other colours too!

- Surgical Care Practitioner (SCP)
- Role: assists in surgical procedures and provides critical pre- and post-operative care.
- Responsibilities: plays a key role in patient management and support the surgical team.
- Advanced Nurse Practitioner (ANP)
- Role: plays a key role in patient management and supports the surgical team.
- Responsibilities: daily monitoring of your condition and updating the rest of the team on your progress.
- Senior House Officer (SHO)
- Role: a junior doctor responsible for daily monitoring of your condition and updating the team on your progress. Please note – may wear other colours too!

- Ward Nurse
- Role: looks after you and other patients on your ward bay.
- Responsibilities: helping with day-to-day essential needs, monitoring your vital signs, administering medications.

Team members you may also meet
- Ward Sister
- Role: senior nurse in charge, responsible for the overall running of the ward and maintaining nursing care standards.

- Physiotherapist
- Role: helps with physical recovery after surgery.
- Responsibilities: designing and guiding through rehabilitation exercises, improving mobility, and promoting heart health through physical activity.

Pharmacist
- Role: manages and reviews medication.
- Responsibilities: ensures safe medication practices, advising on drug interactions, and tailoring medication plans to individual needs
Students
There may also be students present on the ward rounds to observe and gain learning opportunities.



Cardiac Intensive Care Unit (CICU)
- CICU ward rounds can be more complex and often have a team discussion in addition to the ward rounds.
- This is typically during the times when teams are swapping over shifts.
- Key information about each patient is discussed, without engaging the patient in the discussion, to ensure everyone is up to date.
Glossary
During the ward round you may hear the team mentioning some specialist terms, particularly whilst examining you:
- Arrhythmia: an abnormality in your heart’s rhythm
- Antihypertenive: a medication used to lower your blood pressure
- Beta-blockers: a medication used to slow down your heart
- Blood Pressure: the measurement of the force of blood inside your arteries. Each time your heart beats, it pumps blood into arteries, which carry blood throughout the body
- Electrocardiogram (ECG): a non-invasive test used to record the heart’s electrical activity and can help us see if your heart is working properly
- Oedema: a sign that might be picked during examination (commonly around the ankles) and suggests a build up of fluid in the body’s tissues
- Observations (Obs): these are measurements including your heart rate, breathing rate, blood pressure, temperature and oxygenation levels
- Sternum (or breastbone): long flat bone located at the front of your chest, we check if this is secure (‘stable’) after open heart surgery
Cardiac Intensive Care Unit (CICU) and Cardiothoracic High Dependency Unit (CHDU)
Following your operation you will be taken to the cardiac intensive care unit (CICU). During your stay in the CICU or CHDU you will be monitored very closely. After your surgery you will be kept asleep until the doctors and nurses are happy that your condition is stable.
You will be sedated and a machine will help you to breath. This is called a ventilator. Once you are ready to breathe on your own you will be allowed to wake up and weaned off the ventilator. When you are stable enough, you will be moved to the high dependency unit and then to the ward.
Recovery
Your operation is unique to you, and everybody recovers differently, but below is a typical timeline of the recovery for a patient. Please remember that you will recover at your own pace. It is important not to compare your progress with that of other patients.
Day one
Your progress post operatively will be monitored closely. Your urine output, drainage into the chest drains and blood tests will all be observed frequently.Your chest drains are likely to be removed the morning after your surgery.
It is very important to maintain good oxygen levels after your surgery to help your body heal, therefore it will be necessary for you to wear an oxygen mask for the first day or so.
The physiotherapist will see you in CICU and go through your deep breathing and circulation exercises. You will be given breakfast and may be assisted into a chair on day one post operatively.
Day two
If you continue to make good progress and are not requiring support from certain medicines or have high oxygen requirements, we will remove your remaining lines and tubes.
You will be assisted out of bed again and will be seen by a physiotherapist. It is expected that you will be able to walk with supervision for short distances, for example to the bathroom. We would hope that you will have resumed your normal diet by this point.
You may have some routine checks performed which will include an ECG and blood tests.
Days 3 to discharge
Under the supervision of the nurses and physiotherapists you will gently increase your mobility day by day. By day three you may be mobilising along the ward corridor.
If appropriate you will spend some time on an exercise bike and climb the stairs with the physiotherapist in preparation for discharge. If you have not had your bowels open, please ask for a laxative.
If you have had a valve replacement or repair, you will require an echocardiogram after your surgery, ideally this would happen before you go home but it may be done on or before your six week clinic review. Your discharge plans will be discussed, please speak to your friends and family about how they can help you when you go home and to arrange transport home.
For patients from the South Tees area, you will be seen by a rehabilitation nurse to discuss cardiac rehabilitation classes. If you are not from this area your details will be passed on to the appropriate service local to you.
Medication you need to take home will be ordered. On the day of discharge you will be given a letter to deliver to your GP with information regarding your hospital stay.
Physiotherapy following heart surgery
Physiotherapy following heart surgery is very important. After your surgery, your lungs are less inflated and you may have some phlegm. It is important that you re-inflate your lungs and clear any phlegm in order to avoid a chest infection.
Our physiotherapist will visit you in the CICU once you are awake and start your physiotherapy and will continue every day until you are discharged. You will be given advice on regular exercise at home during discharge.
Going home
What will be arranged?
Tablets to take home
You will be given a 4 weeks’ supply of tablets to take home on the day of discharge if you do not have your own supply. The hospital does not supply medications that can be bought over the counter as your local Pharmacy. If you are able to take Paracetamol, it would be a good idea to have a supply available at home ready for when you are discharged. You will need to obtain a repeat prescription from your GP. The nurse discharging you will go through your medicines with you, they will explain what they are for, how long to take them and how or when they will be reviewed.
INR clinic
This will need to be arranged if you are being discharged home on Warfarin. Not all GP practices monitor INR levels in which case the ward will refer you to your local hospital.
It would help the nursing staff if you found out from your GP before your admission to hospital as to assist with the discharge planning.
District Nurse or Practice Nurse
If you require a dressing change, or stitches removed, then the district nurse or practice nurse visit will be arranged by the ward before you leave. Wounds are often dry and healing well at time of discharge therefore do not always require a dressing.
GP letter
This letter will be given to you to take to your doctor’s surgery. It gives a brief summary of your hospital stay and the type of operation that you had and also a list of the tablets that you are now taking.
Try to take it as soon as possible to your GP as you will need to arrange a repeat prescription for your tablets. If you are staying at a different address to your own, then you will need to register as a temporary patient at a GP surgery for that address.
Outpatients’ follow up appointment
These will be made for you by your consultant surgeon’s secretary approximately 6 weeks after your surgery. You will be contacted by one of the Advanced Nurse Practitioner team to talk about your recovery. This will be done over the telephone in the first instance. Should you or the Nurse Practitioner have any concerns, we may invite you back to our outpatient department to be seen in person.
Sick note
If required, this can be obtained before you leave the ward, please ask your nurse if a sick note is required.
Transport
Please arrange your own transport home.
You can safely ride in a car and you must continue to wear a seat belt. Having a folded towel available in the car to put between your chest and the seat belt can make your journey more comfortable.
Support services
If at time of discharge you are not fully independent, we can liaise with social work and, or support services to organise care at home (that does not include shopping or house work). If you are a carer for someone, please organise for someone else to take over this role or respite temporarily.
What to expect?
Going home is the next step on the road to recovery following heart surgery.
These guidelines have been written to anticipate most of the questions that are likely to crop up over the next few weeks. Remember these are guidelines. People recover at different speeds and it is very common to have good days and not so good days.
The anticipation of going home is often combined with apprehension about leaving the security of the hospital and you may find it takes a little while to settle down. There may be a feeling of anticlimax and your partner may feel that it is a traumatic time, for example, leaving you on your own for the first time. These are very natural feelings which will subside as you settle back home.
Do not worry if you feel irritable or emotional at times, or experience mood swings in the initial stages. Some people also find that their concentration is not good to begin with. These are fairly common problems and will improve. Try to take one day at a time.
The aim of your operation is to improve your quality of life and get you fitter than before. As your strength returns, you will want to do more and should be encouraged to do so.
Pain
For most heart operations the breastbone is divided and therefore will take a number of weeks to heal properly. During this time (up to 8 to 12 weeks and in some cases longer) it is common to experience aches and pains in the chest, back and shoulders.
A painkiller, for example, paracetamol, should be taken to relieve this and is usually effective when taken as prescribed, 4 times a day. You should be able to cough and hold yourself tall without too much discomfort. Some people may also experience pins and needles in their fingers.
If you have any concerns or need stronger painkillers, you need to consult your family doctor. You should be aware that some painkillers cause constipation. Remember to drink plenty of water and eat fresh fruit.
If laxatives are required, please discuss with the ward nurse before leaving hospital or your GP.
Shortness of breath
Most patients experience mild shortness of breath on exertion after surgery, which is normal, and should improve as your recovery progresses. If this happens at rest or does not improve you should contact your GP.
Lifting
As your breastbone is healing, you must be careful not to put it under undue strain. Avoid lifting, pushing or pulling heavy objects – more than 8 to 10 pounds (approximately half a kettle of water) for 6 weeks, also awkward reaching and straining. This includes for example, no ironing, hoovering, or carrying shopping. Use both hands and turn to face whatever you are trying to move.
Light activities are allowed, for example, washing up, light cooking etc. Stick to light household tasks initially build things up gradually.
Rest
You will probably feel weak initially and tire quickly. Take care to build things up gradually with plenty of sleep, including an afternoon nap if needed. Try to get a balance between activity and rest. You may need to limit the number of visitors you have when you first go home.
Sleep
Sleep and rest are important. Try to keep a day and night routine and sleep however you feel most comfortable. For the first four weeks it is recommended you sleep on your back. Try to move your position slightly throughout the night. Initially you may find it more comfortable to sleep in a more upright position than usual using extra pillows for support.
Exercise
This will be discussed with you by the physiotherapist before you leave hospital. Please refer to your physiotherapy booklet which provides a rough guide to an exercise programme. Exercise will help you and your heart get fitter if carried out carefully and sensibly.
Sexual relationships
These may be resumed when you feel ready. You and, or your partner may feel apprehensive initially – this is perfectly normal. Try to choose a comfortable position to begin with that does not put too much pressure on your chest – a less active role is preferable – and do not be afraid to discuss your fears with your partner.
Avoid intercourse soon after a heavy meal and try to find a time when you feel rested and relaxed. If you encounter any difficulties in this area, it could possibly be connected with your tablets in a small number of cases. If in doubt consult your doctor.
Eyesight
It is very common to experience visual disturbances for the first 6 weeks after your operation. People wearing glasses may find that their vision is variable and their glasses do not seem to work as well as they did before.
This is a temporary situation and it is therefore inadvisable to consider having your glasses changed in the first 4 to 6 weeks after surgery.
Hygiene
You are able to take a shower or bath (preferably a shower initially) once your wound is dry and healing. Try to avoid extremes of temperature and wash gently around the wound site.
Wounds
If you develop a temperature or notice any redness, tenderness or discharge around the wound site, contact your GP who will prescribe the appropriate treatment or refer you back to us if necessary.
If you have a leg wound, you may experience more discomfort from your leg than your chest. There may be a small area of numbness or pins and needles around your ankle which usually resolves with time. This is due to a division of nerves situated close to the vein in that area. You may also experience swelling of the foot and ankle of the affected leg.
When you are not walking around, try to sit with your leg up at least level with your body, preferably higher.
We advised women to wear a comfortable soft bra or sports bra after surgery. This provides an additional support which helps with healing of chest wound.
Anti-coagulation therapy
People with a mechanical valve will need warfarin for the rest of their life. It is very important before you leave hospital to understand your warfarin, how long you need to take it, where and when you need to have your blood checked, and what the warfarin level should be.
Other conditions that develop after heart surgery like an irregular heartbeat called atrial fibrillation or flutter can require a different type of anti-coagulation medication. If this is required, you will be given some information and safety card to carry with you by our pharmacy staff.
Infection (valves)
If you have a temperature or any sign of infection it is important to see a doctor and remind them that you have had a heart valve replaced. This is due to the small possibility of the infection being related to the valve.
Dentist
It is important for anyone with a valve surgery to have regular (at least 6 monthly) dental checks because of the possible risk of infection. Make sure your dentist knows you have had a heart valve replacement – Your surgeon would have advised you whether you need to have antibiotics before your dental treatment.
Work
Many people return to work after approximately 3 months. This will depend on your recovery and your type of work. Planning a phased return to work on light duties, if possible, is a good way to ease back into work.
Driving
Ordinary licence
If you drive a car, moped or a motorcycle (group 1) and you have had routine heart surgery without complications the DVLA state that you must not drive for 1 month. You do not need to inform the DVLA and you should have your doctor’s approval before starting to drive. Your insurance company may have different rules to the DVLA so let the company know that you’ve had heart surgery.
HGV licence
If you have an HGV licence, speak to your hospital doctor and cardiac rehab nurse. You must contact the DVLA.
Flying
If you are planning a holiday abroad, check with your doctors as to when they are happy for you to fly. The cardiac rehab nurses have information on insurance, which they will give you when you attend the program.
If you have a pacemaker, report to someone at the airport to avoid the archway metal detectors as it may trigger off the alarms. The amount of metal contained in a heart valve or the stainless steel wires in your chest on their own will not trigger the alarms. However, these combined with other metal items you may be carrying may be enough to activate the alarm system. If in doubt, speak to an airport official before walking through the detector.
What should I do if I have a problem?
If you have a problem that is related to your admission or hospital stay or you develop a wound problem please contact the ward.
For any other issues contact your GP, if your GP is closed and you feel it is urgent, you can go to your nearest accident and emergency department or dial 999.
Useful contact numbers
- Ward 32
Telephone: 01642 854532 - Cardiac High Dependency Unit (CHDU)
Telephone: 01642 854532 - Cardiothoracic Intensive Care Unit (CICU)
Telephone: 01642 282676
If you require further information please contact the Cardiac Specialist Nurses on the below details:
Telephone: 01642 282507
Email: [email protected]
Patient experience
South Tees Hospitals NHS Foundation Trust would like your feedback. If you wish to share your experience about your care and treatment or on behalf of a patient, please contact The Patient Experience Department who will advise you on how best to do this.
This service is based at The James Cook University Hospital but also covers the Friarage Hospital in Northallerton, our community hospitals and community health services.
To ensure we meet your communication needs please inform the Patient Experience Department of any special requirements, for example; braille or large print.
T: 01642 835964
E: [email protected]