Cardiothoracics
You have been found to have a condition called mitral regurgitation, and your doctors are considering treating this by a procedure to repair the mitral valve using a trans-catheter technique.
This involves placing a clip onto the leaking heart valve. There are several different types of clip available and at The James Cook University Hospital we most commonly use the MitraClip device.
We want you to be fully informed and involved in the decisions made about your care – this leaflet aims to enhance the information given to you so that your heart team ensures you receive the best possible care.
What is mitral regurgitation?
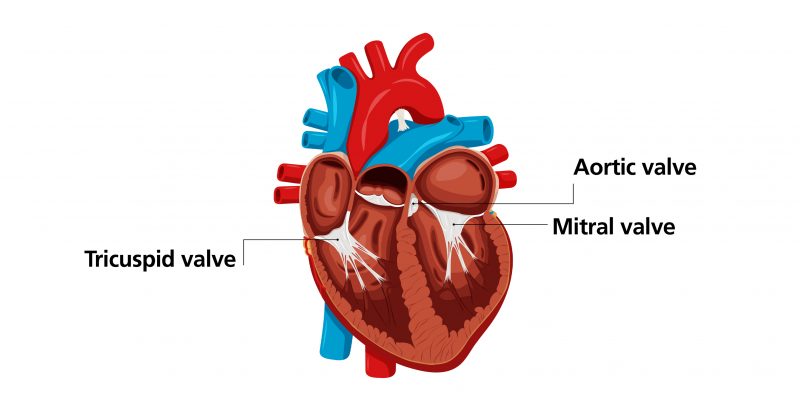
The mitral valve is one of the four heart valves that control the flow of blood in and out of the heart. If the valve becomes abnormally leaky it is called mitral regurgitation. Without treatment, mitral regurgitation usually worsens with time.
Although medicines can slow the progression of mitral regurgitation, the effects of long-term mitral regurgitation can result in symptoms of:
- Breathlessness
- Fatigue
- Fluid over-load
What treatment is available?
Until now mitral valve repair has involved open-heart surgery. As your doctor will have explained, we believe you may be at high risk for this surgery or there are reasons it may not be suitable for you.
However, you may be suitable for another form of valve repair, where the valve is repaired through the blood vessels in the groin. At the moment this type of treatment is only appropriate for certain patients.

If you do not want to have an operation of any type, we can use medication to manage your condition but this will only control symptoms temporarily and does not deal with the underlying problem.
What tests will I need?
Before you have your valve repair procedure, we will carry out a number of tests to find out as much as we can about your heart and so help us carry out the valve repair effectively.
These include:
Routine blood tests
An ECG (electrical trace of the heart)
A transthoracic echocardiogram (ultrasound scan of the heart)
A trans-oesophageal echocardiogram (TOE)
This is a more detailed ultrasound scan of the heart where you are asked to swallow a thin tube which is used to look at the heart.
In some circumstances additional tests will be required.
These may include:
An angiogram (an x-ray test in which thin plastic tubes are inserted into the blood vessels at the groin or wrist under local anaesthetic. Dye is injected through the tubes to show up the blood vessels around the heart and main blood vessels down to the groin area).
Lung function tests (breathing tests by blowing into a small tube)
These tests will be carried out in the weeks or months leading up to your procedure. They may be carried out in different hospitals and you will be advised about them by letter.
How is the TMVr procedure performed?
Transcatheter valve repair is carried out in the cardiac catheterisation laboratory under general anaesthetic, so you will be asleep for the duration of the procedure.
Once you are asleep, we will pass a trans-oesophageal echo (TOE) probe into your oesophagus (also known as your gullet or “food pipe”). This allows your cardiologist to guide the catheters into place in your heart.
We will make a small incision (cut) in your groin and then, through the incision, insert a small tube. Through this tube we insert a catheter. Using x-ray pictures, we then guide this catheter into your heart.
To access your mitral valve a small puncture is made in the interatrial septum, the thin wall between the two upper chambers in the heart. Once the catheter is in place we can deliver the clip into position to repair the leak of the mitral valve. Some patients may require more than one clip to adequately repair the valve.
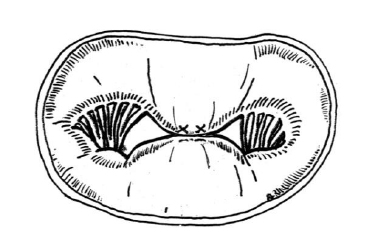
The clip pulls the centre of the mitral valve together. This reduces the amount of leak through the valve and means that the valve has two openings to allow the blood to flow through.
What are the risks of the procedure?
As with any operation, there is a risk of complications from this procedure. It is important to remember, though, that your doctors would not have recommended having this procedure if they did not believe the potential risks to be outweighed by the likely benefits to your health.
Your doctor will discuss these risks with you in more detail as they may change according to your clinical condition.
TMVr is a relatively safe procedure but there is a small risk of serious complications (approximately 5%) which can include:
- Bleeding into the sack around the heart
- Bleeding requiring blood transfusion
- Damage to the blood vessels requiring surgical repair
- Partial or full detachment of the device after implantation
- Narrowing of the heart valve following clip deployment
- Damage to the valve making the valve leak worse
- Heart rhythm disturbance
- Damage to the walls of the heart
- Residual connection between two chambers of the heart (atrial septal defect)
- Death
- Stroke
- Heart attack
- Kidney failure
- Infection
- Need for emergency open cardiac surgery
What are the benefits of the procedure?
This procedure aims to reduce the leak through the mitral valve, and improve the symptoms of heart failure such as breathlessness and fatigue.
A successful procedure will reduce the risk of fluid build-up leading to hospital admission and in some cases may improve prognosis (make you live longer).
Before the procedure:
It is important that your stomach is as empty as possible before the anaesthetic.
- Usually you must not eat or drink anything at all for six hours before your procedure.
- You may also be asked to with-hold some of your medications a number of days before you come into hospital.
The team will advise you further if this is the case.
After the procedure:
After the procedure you will be taken to the coronary care unit for observation. Once you are stable, you will be moved to a general cardiology ward.
Before you go home you will be given advice about recovery from the team. You will be able to return to your normal activity fairly quickly but it is not unusual to feel tired or “washed out” for a few days. You may continue to feel short of breath to begin with but this should improve with time.
The DVLA advises that you should not drive for four weeks after your procedure. You do not need to inform the DVLA (unless you hold a group 2 license) but you should inform your insurance company.
There may be bruising at the groin area where the tube was inserted during your procedure. This may feel tender but should settle within a few days.
Important
Please seek medical advice if you experience any of the following:
- Any unusual pain, swelling or bleeding at the entry site
- Any discolouration, tingling, pain or loss of sensation in your legs
- Increased swelling in your ankles
- You are feeling very dizzy or lightheaded
- Any signs of an infection or abnormal rise in temperature.
Follow up:
You will have a follow up appointment around 6 to 8 weeks after the procedure. You will also have another echocardiogram (ultrasound of the heart) to check the function of the repaired valve.
Long term follow up will be organised thereafter and may be arranged locally.
Contact us
During office hours
If you need more information please contact the Structural Heart Specialist nurse
Telephone: 01642 854239
Mobile: 07741 616394
Out of hours
If you need urgent advice following discharge from hospital, you can speak to a member of staff on the Coronary Care Unit 24 hours a day on 01642 854801
Patient experience
South Tees Hospitals NHS Foundation Trust would like your feedback. If you wish to share your experience about your care and treatment or on behalf of a patient, please contact The Patient Experience Department who will advise you on how best to do this.
This service is based at The James Cook University Hospital but also covers the Friarage Hospital in Northallerton, our community hospitals and community health services.
To ensure we meet your communication needs please inform the Patient Experience Department of any special requirements, for example; braille or large print.
T: 01642 835964
E: [email protected]